

About Parathyroid Disease and Hyperparathyroidism; Hypercalcemia
Hyperparathyroidism is a hormonal problem that can develop at any age, but occurs most commonly in postmenopausal women (2% of older women and 1% of older men). It develops because of excessive secretion of parathyroid hormone (PTH), an important factor in calcium metabolism. It can lead to high PTH levels and calcium levels in the blood, and a wide range of symptoms.
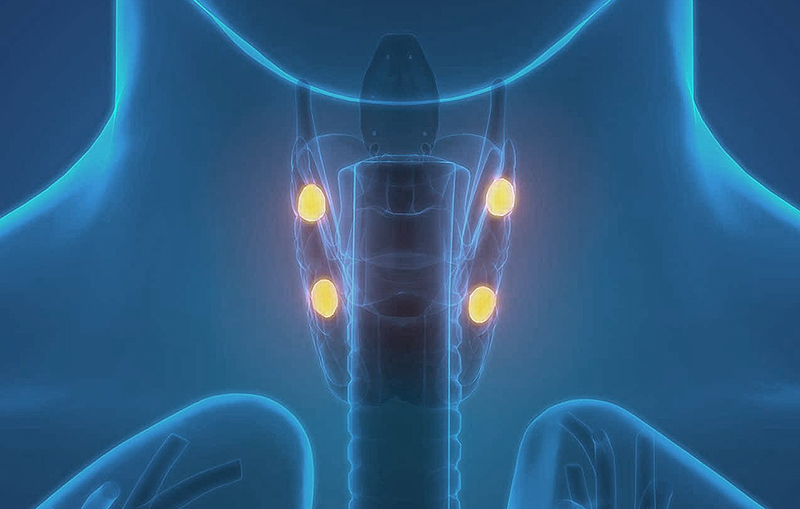
What is the Parathyroid Gland and its function?
Most people are born with four parathyroid glands located behind the thyroid at the lowwer part of the neck. These glands produce PTH in the bloodstream which controls calcium levels, raising levels when they are too low. It’s impact can affect bones, intestine, and the kidneys. A normal parathyroid range is between 9.0 and 10.1. If the level of parathyroid hormone is too high, the result is hyperparathyroidism.
Primary Hyperparathyroidism
When an abnormal parathyroid gland ‘goes rogue’ and stops responding to normal signals from the body, it tells the body unnecessarily that it needs more calcium. Calcium is then leached from the bones (a cause of osteoporosis) and intestines to compensate, and can be deposited in the kidneys, which leads to kidney stones. A build-up of too much calcium in the bloodstream can be either asymptomatic or can lead to a variety of problems.
Some patients with a parathyroid tumor have normocalcemic hyperparathyroidism where the calcium level is normal but the PTH is high. Other patients may have high calcium but high-normal or normal PTH levels. Assuming that there are no other causes of high calcium or high PTH, these patients should have their primary hyperparathyroidism treated. The cause of overactive parathyroids in 1% of patients is inheritance of a gene abnormality from one parent. The cause of a parathyroid tumor in the other 99% of patients is usually unknown, although radiation therapy to the face or neck can be a factor in causing a single parathyroid tumor.
Dr. Melanie Goldfarb, Director of Center for Endocrine Tumors and Disorders, and Associate Professor of Surgical Oncology of Saint John’s Cancer Institute, explains primary hyperarathyroidism in simple terms, how it affects the body, who should be screened, and treatment.

Secondary Hyperparathyroidism
Secondary hyperparathyroidism occurs when a disease unrelated to the parathyroids causes all of your parathyroid glands to become enlarged and overactive. The most common cause of secondary hyperthyroidism is kidney failure, which can lead to overstimulated parathyroid glands due to lower levels of calcium in the bloodstream.
Prolonged vitamin D deficiency is the second most common of secondary hyperparathyroidism, followed by gastrointestinal malabsorption, such as after a gastric bypass procedure.
Tertiary Hyperparathyroidism
Tertiary hyperparathyroidism occurs when secondary hyperparathyroidism develops into primary hyperparathyroidism. For example, a kidney failure patient who has received a kidney transplant is later diagnosed with primary hyperparathyroidism.
Once the clinician has validated tertiary hyperparathyroidism, then the statistics are the same as primary hyperparathyroidism, where most people have a single overactive parathyroid gland. If however, the secondary hyperparathyroidism was never cured and renal insufficiency (advanced loss of kidney function) still exists, then these patients likely have disease in all four of their parathyroid glands.
Signs and Symptoms of Hyperparathyroidism and Hypercalcemia
Hyperparathyroidism, or hypercalcemia, can be asymptomatic (not having any symptoms), cause mild symptoms, or in rare cases, present severe symptoms. The most easily recognized and curable primary hyperparathyroidism/hypercalcemia symptoms are osteoporosis and kidney stones.
Common symptoms of high calcium or high PTH:
Nervous system
- Mood swings
- Depression
- Forgetfulness
- Irritable
- Concentration problems
- Fatigue
- Decreased sexual desire or impotence
Kidney/Urinary
- Kidney Stones
- Nocturia (going to the bathroom a lot at night)
- Worsening kidney function
Digestive system
- Stomach or duodenal ulcer
- GERD (reflux)
- Pancreatitis
- Abdominal pain
- Constipation

Musculoskeletal
- Bone pain
- Joint pain
- Bone fractures
- Osteoporosis
- Generalized weakness
Diagnosis of Primary, Secondary, and Tertiary Hyperparathyroidism
Since hyperparthyroidism is a hormonal problem, a diagnosis is reached by measuring the hormone levels in the body, such as calcium and PTH.
Common blood tests for parathyroid disease:
- Calcium
- PTH (parathyroid hormone)
- Vitamin D 25-OH and vitamin D 1,25-hydroxy
- Creatinine
Once a diagnosis of primary hyperparathyroidism has been made and a surgeon has evaluated you for parathyroid surgery, parathyroid Imaging will be performed. This may include a parathyroid ultrasound, 3D parathyroid CT scan, or less commonly a Sestamibi scan. The endocrine surgeon will perform a parathyroid ultrasound in the office and order additional testing as needed.
Other tests may order include:

- Bone Scan
- 24-hour Urinary calcium
- Abdominal CT (to look for kidney stones)
Many clinicians may not identify parathyroid disease when mildly elevated calcium levels exist (hypercalcemia), inclduing complaints such as fatigue, forgetfulness, problems with concentration, depression/anxiety, kidney stones or disease, osteoporosis, constipation, stomach ulcers, or sexual dysfunction.
Additionally, primary care physicians may not refer patients for minimally invasive surgical treatment that could cure them of their parathyroid disease if they beleive the parathyroid condition is mild.
Treatment of Primary, Secondary, and Tertiary Hyperparathyroidism
The only cure for hyperparathyroidism is parathyroid surgery–the removal of one or more parathyroid tumors (parathyroidectomy).
During parathyroid surgery, the number of parathyroid glands removed will be determined by measuring parathyroid hormone (PTH) in the blood during the operation. Most parathyroid surgery is minimally invasive (small incision). Parathyroidectomy (parathyroid removal) may be recommended based on your situation and health history.
Benefits of having parathyroid surgery include:
- Improved bone density and decreased risk of bone fractures (stabilization of osteoporosis)
- Improved quality of life
- Lower risk of kidney stones (up to 90 percent of patients do not develop any new stones)
- Decreased risk of premature death
- Disappearance or improvement of symptoms
Parathyroid Cancer
Parathyroid cancer is a rare cause of primary hyperparathyroidism, which is very difficult to diagnosis before surgery. Typically, patients will have very high calcium and PTH levels. During parathyroid surgery, the parathyroid tumor is usually dense and stuck to the surrounding tissues, as wells as the thyroid gland. Parathyroid cancer survival is generally expected because this type of tumor is very slow-growing. However, because it can recur, patients may need re-operations in the future.
What to Expect After Parathyroid Surgery
If you have questions regarding Parathyroid and Hyperthyroidism, please call today. Request an appointment
Melanie Goldfarb, M.D., M.Sc., FACS, FACE
Director, Center for Endocrine Tumors and Disorders
Medical Director for Cancer Survivorship
Dr. Melanie Goldfarb is a fellowship-trained endocrine surgeon and Director of the Center for Endocrine Tumors and Disorders. Her expertise is minimally invasive surgery for thyroid cancer and disorders, hyperparathyroidism, and adrenal tumors, including pheochromocytoma, Cushings, Conns, and adrenal cancer.




